Understanding Hemorrhoids and Your Treatment Options
Hemorrhoids are very common and can cause bright red bleeding, itching,
pelvic pressure, or painful lumps. While not dangerous, they can
significantly affect daily life.
Traditional treatment starts with lifestyle changes, such as a high-fiber diet,
increased water intake, sitz baths, or topical creams. Rubber band ligation
and other center procedures are effective but can be uncomfortable and
involve direct contact with sensitive tissues.
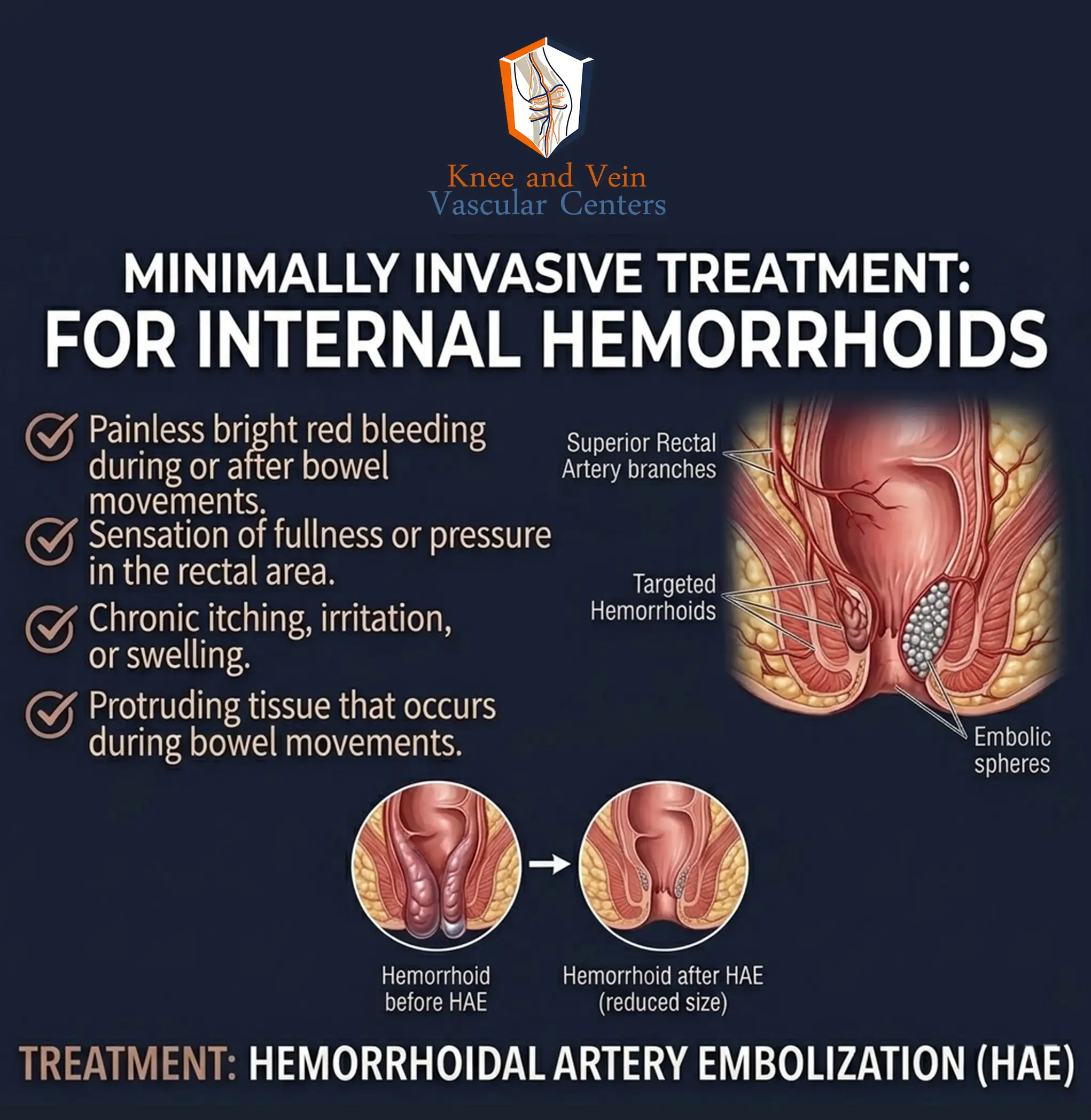
We specialize in Hemorrhoidal Artery Embolization (HAE), also called
Emborrhoid—a minimally invasive outpatient procedure that avoids anal
incisions. Using a tiny catheter, we block the blood flow feeding internal
hemorrhoids, causing them to shrink and stop bleeding naturally. Most
patients return to normal activities within 1–3 days.
HAE is ideal for patients with internal hemorrhoids (Grades I–III) who want an
effective, low-pain solution without traditional surgery.
Ready to take the next step?
Explore the tabs below to learn more about your options. If you’re ready to
take control of your health, schedule your appointment online or call our
center - we’re here to help you get back to your life.
Understanding Hemorrhoids & Your Symptoms
What Are Hemorrhoids?
Hemorrhoids are swollen blood vessels in and around the anus and lower rectum. By age 50, about half of all adults have experienced hemorrhoid symptoms.
Types of Hemorrhoids:
- Internal: Inside the rectum; usually painless but can bleed
- External: Under the skin around the anus; can be painful, especially if a clot forms
Symptoms:
- Bright red blood on toilet paper, stool, or in the toilet
- Itching or irritation around the anus
- Pain or discomfort, especially with external hemorrhoids
- Swelling or a lump near the anus
- Mucus discharge
- Feeling of incomplete bowel movement
Causes:
- Straining during bowel movements
- Chronic constipation or diarrhea
- Sitting on the toilet for long periods
- Low-fiber diet
- Pregnancy and childbirth
- Obesity
- Heavy lifting
- Aging (weakened supportive tissues)
Grading Internal Hemorrhoids (Goligher System):
- Grade I: Bleeding, no prolapse
- Grade II: Prolapse on straining, returns spontaneously
- Grade III: Prolapse requires manual reduction
- Grade IV: Permanently prolapsed, cannot be pushed back
Traditional Treatment Options
Lifestyle & Dietary Measures:
- Increase fiber intake (25–35 g/day) via fruits, vegetables, whole grains, or supplements
- Drink 6–8 glasses of water daily
- Avoid straining during bowel movements
- Exercise regularly
- Maintain healthy weight
- Avoid prolonged sitting on the toilet
Over-the-Counter Treatments:
- Topical creams, ointments, or suppositories with hydrocortisone or witch hazel
- Sitz baths (10–15 minutes, multiple times daily)
- Pain relievers (acetaminophen, ibuprofen)
- Stool softeners
Center Procedures:
- Rubber band ligation: Bands placed at the base to shrink hemorrhoids
- Hemorrhoidal Artery Embolization (HAE)
- Sclerotherapy: Chemical injection to shrink hemorrhoids
- Infrared coagulation: Heat to reduce hemorrhoid tissue
Surgical Options (for severe or persistent cases):
- For severe hemorrhoids or when other treatments fail, discuss options with a surgeon.
Hemorrhoidal Artery Embolization (HAE)
HAE (or "Emborrhoid") is a minimally invasive procedure performed by interventional radiologists to treat symptomatic internal hemorrhoids without surgery.
How It Works:
- Hemorrhoids are supplied by the superior rectal arteries
- Tiny particles or coils block blood flow to hemorrhoidal tissue
- Hemorrhoids shrink and symptoms improve
During the Procedure:
- Small catheter inserted through wrist or groin
- X-ray guidance to target superior rectal arteries
- Procedure takes 45–90 minutes
- Recovery monitoring 1–2 hours; most go home same day
- Return to normal activities in 1–3 days
Effectiveness:
- Technical success: 93–100%
- Symptom improvement: 63–94%
- Bleeding resolution at 12 months: 69–83%
- Patient satisfaction >80%
Recovery:
- Mild pelvic discomfort for 24–48 hours
- No anal incisions or pain
- Return to normal activities in 1–3 days
- Follow-up at 1 month, with possible 3, 6, 12-month visits
Key Advantage:
- Minimal to no pain
- No risk of fecal incontinence
- No disruption to anal anatomy
Am I a Candidate? / Next Steps
Good Candidates for HAE:
- Symptomatic internal hemorrhoids (Grade I–III) with bleeding
- Tried conservative measures without adequate relief
- Prefer minimal pain and rapid recovery
- Not good candidates for surgery due to other medical conditions
- On blood thinners
- Had previous unsuccessful hemorrhoid procedures
Not Ideal Candidates:
- Grade IV hemorrhoids (permanent prolapse)
- Primarily external hemorrhoids
- Thrombosed external hemorrhoids requiring urgent care
- Other anorectal conditions needing surgery
Next Steps:
- Discuss your symptoms with your doctor
- Determine hemorrhoid grade and suitability for HAE
- Consider lifestyle and dietary measures
- Explore HAE as a minimally invasive option between conservative therapy and surgery